Of all the things that can interrupt a surrogacy journey, this is the one that sits almost entirely in your hands — and the one that's easiest to prevent. Between the day you match and the day a pregnancy from your transfer is confirmed, you remain fully fertile. An unplanned pregnancy of your own during that window means stepping away from the match, or facing a decision no one wants to make, and it sets your intended parents back by months and by real money.
The good news: preventing it isn't complicated. There is nothing mysterious about contraception, and you already know most of it. What actually protects you isn't a special method — it's simply keeping the risk in mind. The surrogates who run into trouble almost never do so because they didn't know how to prevent a pregnancy. They do so because, somewhere in the middle of a busy process, it stopped being top of mind.
This guide is about keeping it top of mind.
Key takeaways
- Until a pregnancy from your transfer is confirmed, you are still fully fertile, with proven, demonstrated fertility behind you. Stay protected the entire time.
- The methods are simple; the real risk is forgetting. Being matched, being screened, or being on your cycle medications protects nothing — only contraception does.
- Don't stop your current method early, and clear any change with your coordinator first. Most accidental pregnancies happen in the gap.
- Some methods need timing: IUDs and implants must come out before transfer, and the Depo-Provera shot can delay your cycle by many months.
- If you're ever unsure whether you're covered, ask your Ivy Surrogacy coordinator — no awkwardness, no judgment.
Your proven fertility is an asset — and the reason this window matters
You were chosen, in part, because you've already carried at least one healthy, full-term pregnancy without complications. That's not incidental — it's a core requirement recommended by ASRM for every gestational carrier. Your proven fertility is one of your greatest assets as a surrogate.
It also means something practical: your fertility is established, not theoretical. The same proven track record that makes you a strong candidate is the reason this window deserves your attention. This isn't about distrust, and it isn't a reflection on you. It's biology — and being clear-eyed about it is what keeps your journey on track.
The real risk isn't knowing how. It's remembering to.
Here is the mindset that prevents almost every unplanned pregnancy in this window:
Until you have a confirmed pregnancy from your transfer, treat yourself as fully fertile — because you are.
That sounds obvious written down. In daily life it's easy to lose. You're in the middle of screening, appointments, medications, and paperwork; it feels like you're already "in the process," so it's natural to assume the process itself is protecting you somehow. It isn't. Being matched protects nothing. Starting your medications protects nothing. Only contraception does.
Keep the awareness, and the methods take care of themselves.
Two windows that matter most
There are two stretches where an unplanned pregnancy does the most damage:
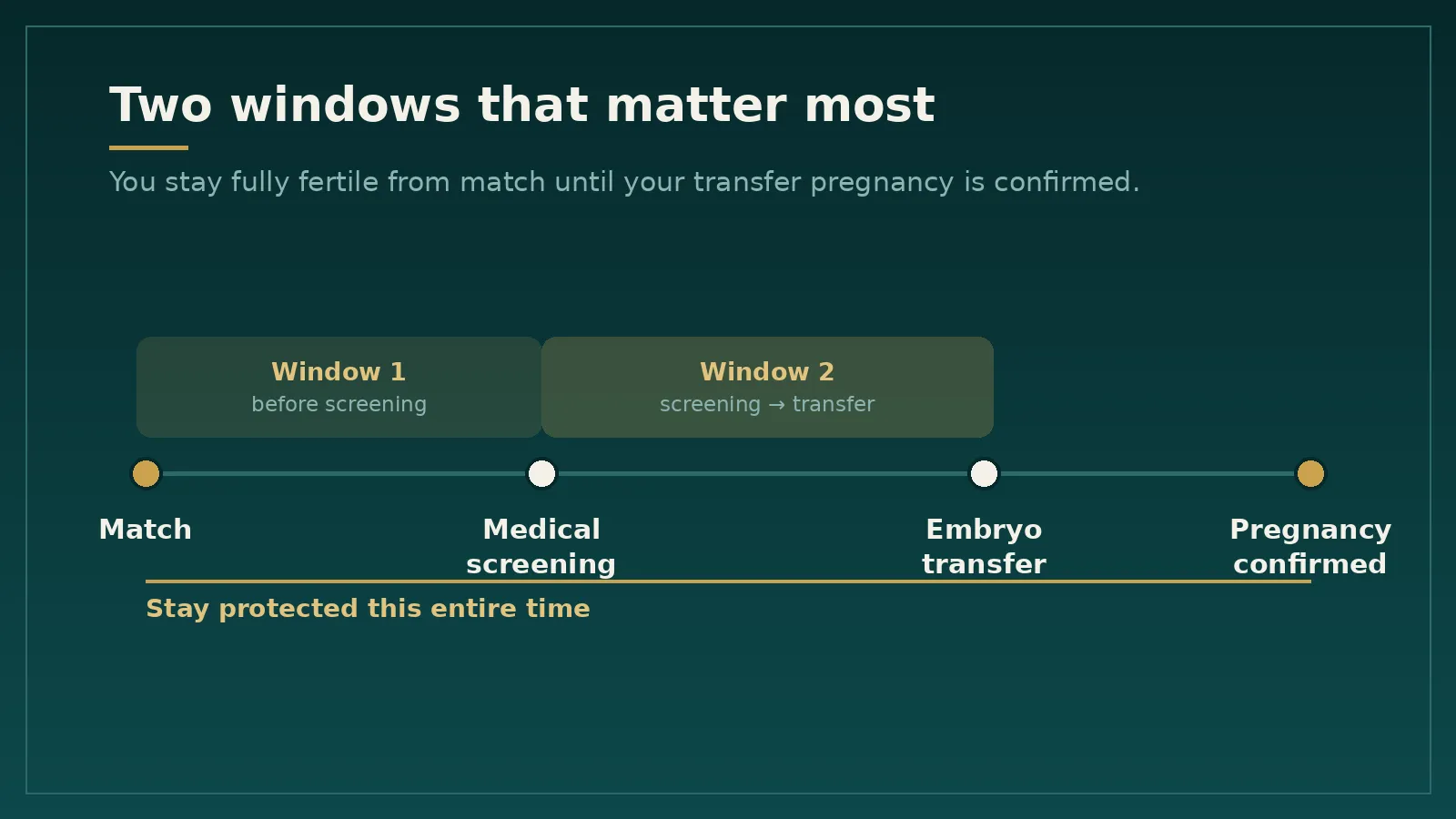
- Before your medical screening. A pregnancy here can disqualify you from the match before it has really begun.
- After you've cleared screening, before your transfer. This is the costlier one. By now your intended parents have committed time and money, your cycle is being planned, and a pregnancy of your own forces you either to withdraw or to end it in order to continue — neither of which anyone wants.
Both windows call for the same thing: steady, deliberate contraception until the transfer pregnancy is confirmed.
What's actually at stake
It's worth being plain about this, without drama. If you conceive your own pregnancy during this window, there are only two paths, and both are hard:
- Carry the pregnancy — which means leaving the match, and your intended parents start over with someone new, months behind.
- End the pregnancy to stay in the journey — a personal, difficult decision that no agency would ever want a surrogate to face unnecessarily.
You've already invested your own time, energy, and a full medical screening. Avoiding this protects your work too, not just theirs.
The simple playbook
One rule covers most of it:
Don't stop your current contraception early, and run any change past your coordinator first.
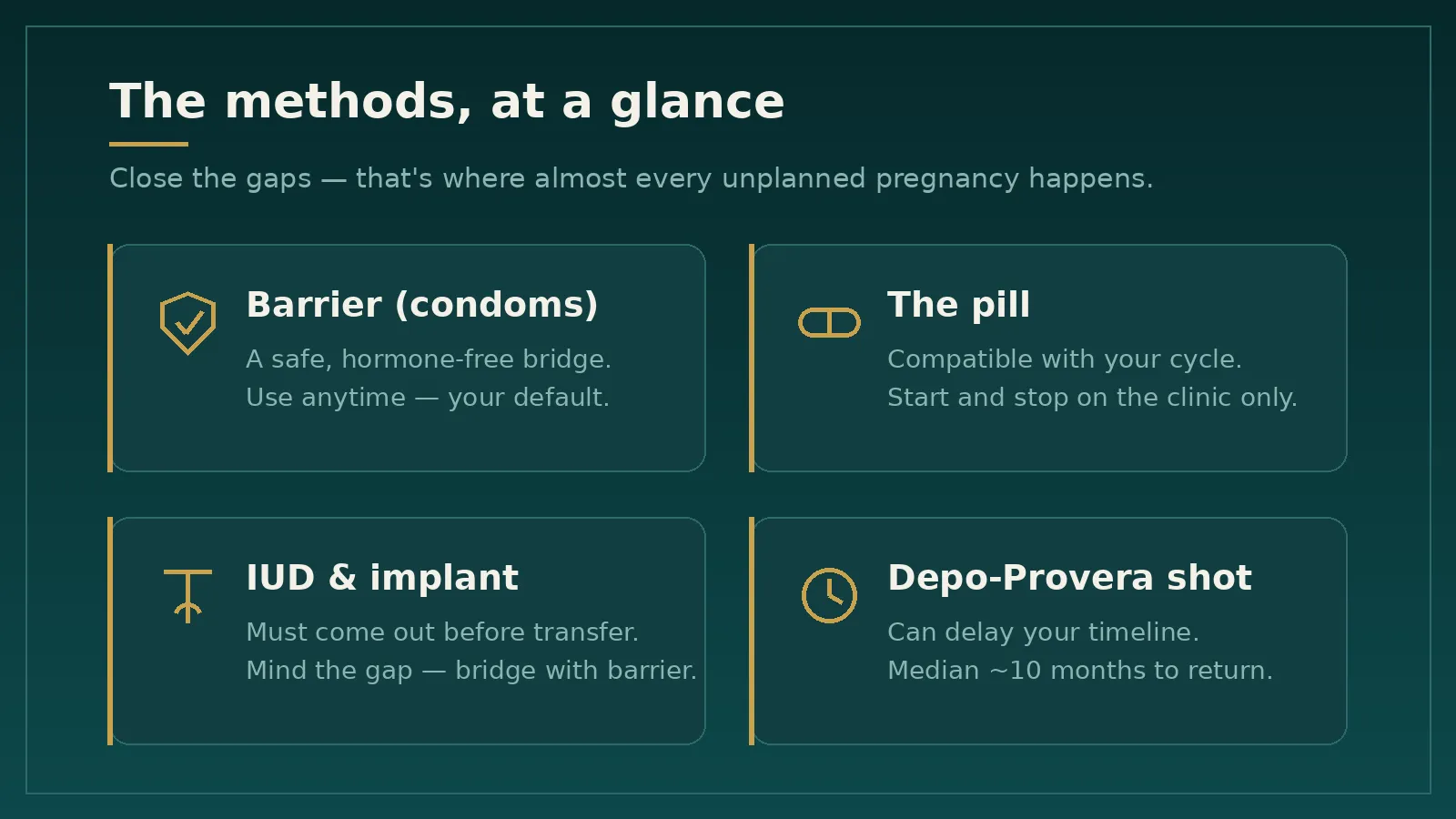
Most unplanned pregnancies happen in a gap — a method stopped too soon, an IUD removed before the cycle is actually locked in, a few "we were careful" weeks that weren't. Close the gaps and you're protected. Here is how the common methods fit:
Barrier methods (condoms). The simplest, safest bridge. No hormones, nothing that interferes with your transfer cycle, available immediately. When in doubt, this is your default.
The pill. Combined birth control pills are fully compatible with a transfer cycle — in fact, clinics often use them to schedule and time a programmed transfer, and in this setting they don't appear to affect transfer outcomes. The key: don't start or stop on your own. Let your clinic tell you when.
IUDs and implants. These have to be removed before a transfer — the procedure can't be performed with an IUD in place. The catch is timing: fertility can return quickly once they're out, so never remove one until your coordinator and clinic confirm the schedule, and use a barrier method in any gap before your cycle locks in.
The shot (Depo-Provera). This one needs a heads-up, because it can work against your timeline. Depo can delay the return of ovulation and fertility for many months after your last injection — by FDA prescribing data, the median time to conception is around 10 months, and for some women it runs longer. If you're on Depo, or thinking about it, tell your clinic early; it may push back when you can start a cycle.
Already had a tubal ligation? Then natural pregnancy is far less likely, and this is largely off your plate. Still, mention it to your coordinator so it's on record.
The transfer window itself. Your clinic will give you specific instructions — usually to use barrier protection or to abstain for a defined period around the transfer. Follow those exactly. They exist both to prevent an accidental natural pregnancy and to avoid anything that could interfere with the procedure or muddy the pregnancy test that follows.
A few things that don't count as protection
- "I'm already in the process." Being matched or screened changes nothing about your fertility.
- "I'm on my cycle medications." The estrogen and progesterone in a transfer cycle are not contraception. You can still conceive.
- "I'm breastfeeding." Not reliable, especially as feedings space out.
- "We were careful / we timed it." Withdrawal and timing are among the least reliable approaches there are — and your fertility is proven.
If any of these has been your quiet assumption, swap it for an actual method.
Frequently asked questions
1. Do I really need contraception if I'm already matched and going through screening?
Yes. Being matched or screened doesn't change your fertility at all. You're protected only by an actual contraceptive method, used consistently until a pregnancy from your transfer is confirmed.
2. What birth control can I use before an embryo transfer?
Barrier methods like condoms are the simplest, hormone-free bridge and work right up to the transfer window. Combined birth control pills are also compatible — clinics often use them to schedule the cycle — but start and stop them only on your clinic's instructions. IUDs and implants have to be removed before transfer, and the Depo-Provera shot can delay your timeline, so plan both with your coordinator rather than on your own.
3. I've started my cycle medications — doesn't that prevent pregnancy?
No. The estrogen and progesterone used to prepare your body for transfer are not contraception. You can still conceive naturally, so keep using your method until your clinic tells you otherwise.
4. When should I have my IUD or implant removed?
Only when your coordinator and clinic confirm the schedule. They have to come out before a transfer, but fertility can return quickly afterward — so use a barrier method like condoms in any gap before your cycle is locked in.
5. I'm on the Depo-Provera shot. Is that a problem?
It can affect your timeline. After your last injection, the median time for fertility to return is around 10 months, and for some women longer — which may push back when you can start a cycle. Tell your clinic early so it can be planned around.
6. Can I have sex during my transfer cycle?
Around the transfer itself, your clinic will usually ask you to use barrier protection or to abstain for a defined period — follow those instructions exactly, both to avoid an accidental natural pregnancy and to keep from interfering with the procedure. Outside that window, intercourse is fine as long as you're using a reliable method consistently.
7. What happens if I get pregnant before my transfer?
It interrupts the journey: you would either step away from the match to carry the pregnancy, or face a difficult personal decision in order to continue as a surrogate. Both set everyone back, which is exactly why this window is worth protecting. If you think you might be pregnant, tell your coordinator right away.
8. Does being a surrogate make me more likely to get pregnant?
Surrogates are selected partly for a history of healthy, uncomplicated pregnancies, which means your fertility is proven and well-established. That's an asset — and it's also why staying consistently protected through this window matters.
Talk to your Ivy Surrogacy team
You should never have to figure this out alone. At Ivy Surrogacy, your coordinator has walked through this exact conversation many times — timing, methods, what your clinic specifically requires — without awkwardness and without judgment. Our team brings a real medical and healthcare background, so when your question touches on medications or your cycle, you're talking with people who understand the clinical side of what you're going through.
If you're ever unsure whether you're covered, that's the moment to reach out — not to guess. Keep the awareness, keep the conversation open, and this risk simply doesn't materialize: a smooth path to your transfer, with nothing standing between you and the family you're helping to build.
Already on your journey? Message your Ivy Surrogacy coordinator with any question, anytime. Thinking about becoming a surrogate? Start your surrogacy journey with Ivy Surrogacy →
Sources
- American Society for Reproductive Medicine. Recommendations for practices using gestational carriers: a committee opinion (2022).
- Oral contraceptive pretreatment does not alter live birth rates in PGT-A screened frozen embryo transfer cycles. Fertility and Sterility (American Society for Reproductive Medicine).
- U.S. Food and Drug Administration / DailyMed. Medroxyprogesterone acetate injectable suspension — prescribing information (return to ovulation and fertility).



