If your surrogacy journey is approaching the third trimester, you may hear your care team mention "induction" — and for many intended parents, the word lands with a jolt of worry. Is something wrong? Is the baby in danger? Who decides? In most cases, the answer is reassuring: in the United States, inducing labor is one of the most routine, well-studied decisions in modern obstetrics, and it comes up often in surrogacy care.
This guide explains what induction actually is, the everyday reasons it happens, why it comes up so often in surrogacy, and — importantly — who gets to make the decision. The short version: induction is common, well understood, and in surrogacy the choice rests with the surrogate and her doctor, not with the agency or the intended parents.
Key takeaways
- Induction means starting labor with medical help before it begins on its own.
- It does not automatically mean something is wrong — it is often planned and proactive.
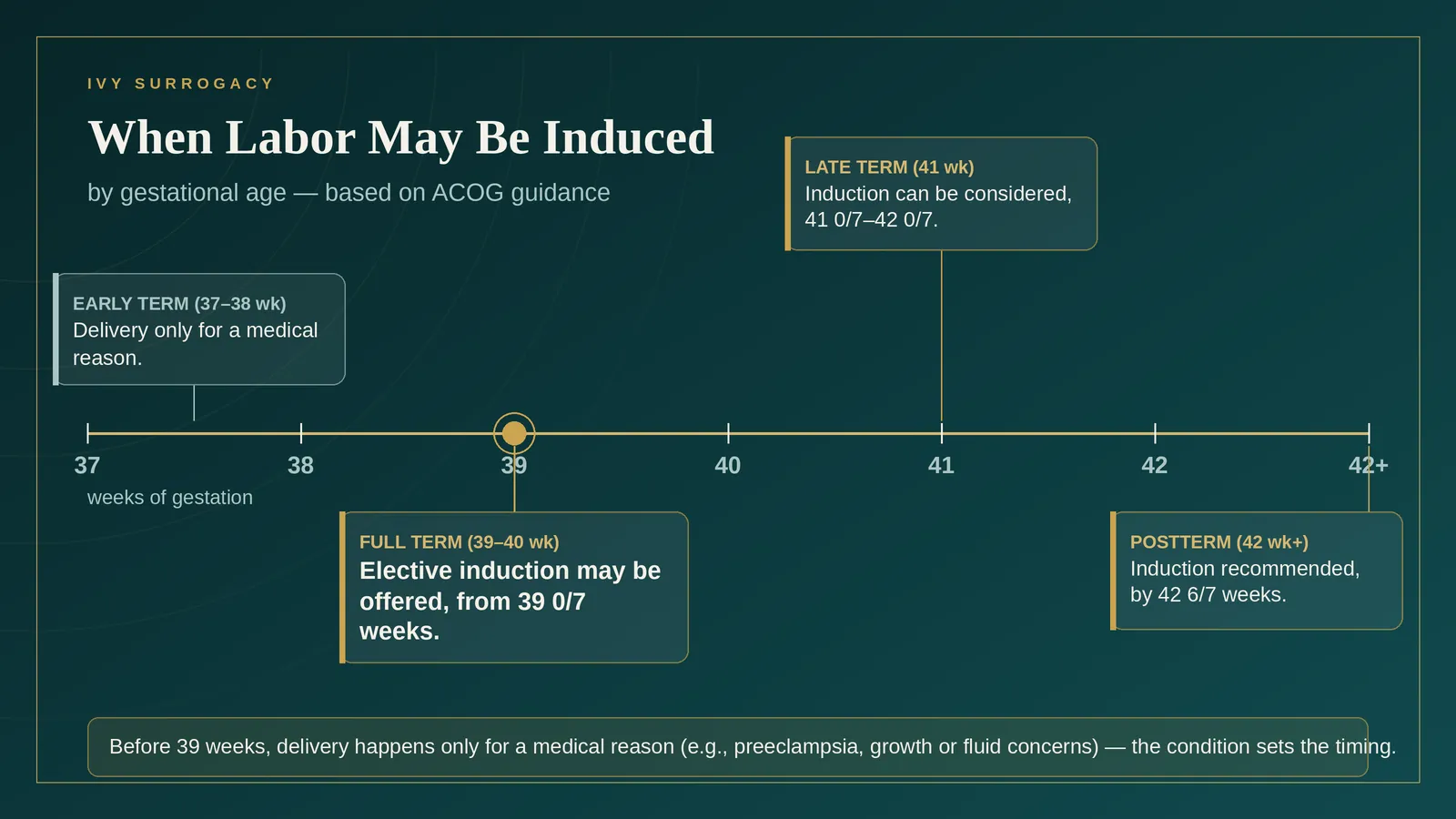
- Elective induction is generally considered only at 39 weeks or later, never earlier.
- Medically indicated induction may happen earlier, when continuing the pregnancy carries more risk than delivering.
- In surrogacy, the gestational carrier and her obstetrician make the medical decisions. Intended parents and agencies do not control the delivery plan.
What "induction of labor" means
Labor induction is the use of medical methods to start labor before it begins on its own. It typically happens in two steps. First, if the cervix isn't yet soft and open ("ripe"), the team helps it along. Then, once the cervix is ready, they stimulate the uterus to contract so the surrogate can deliver vaginally.
This is different from augmentation, which means speeding up a labor that has already started. And it's different from a scheduled cesarean. The goal of an induction is a vaginal birth — just one that begins with a nudge rather than spontaneously.
"Induced" does not mean "something went wrong"
This is the single most important thing for intended parents to understand. A planned induction is not an emergency and usually does not mean the pregnancy is in trouble.
In fact, the largest study on the question pointed the other way. The ARRIVE trial (Grobman et al., New England Journal of Medicine, 2018) randomly assigned more than 6,000 low-risk first-time mothers to either elective induction at 39 weeks or "expectant management" (waiting for labor). Induction did not increase the rate of cesarean delivery — it slightly lowered it (18.6% vs. 22.2%) — and it reduced hypertensive disorders of pregnancy such as preeclampsia (9.1% vs. 14.1%), with no worse newborn outcomes. ARRIVE studied first-time mothers rather than gestational carriers specifically, so its figures do not transfer one-to-one. But it reshaped how U.S. obstetrics views planned 39-week induction: offered to the right patient, it does not appear to raise the risk of cesarean, and may lower it.
So when induction is discussed, it is often a proactive, evidence-based plan rather than a reaction to a crisis. It does not automatically mean there is an emergency. Sometimes induction is elective and planned; other times it is recommended precisely because, at that point, delivering is safer than continuing the pregnancy.
Why induction is so common in the U.S.
Induction has become steadily more frequent in American obstetrics. In 2024, labor was induced in about one in three U.S. singleton births (34.5%) — up from one quarter (24.9%) in 2016, and from fewer than one in ten births in 1989. In other words, an induced birth is now closer to the norm than the exception.
Two broad categories explain almost all of it:
1. Medically indicated induction. Here, continuing the pregnancy carries more risk than delivering, so the team recommends getting the baby out. The timing depends entirely on the condition.
2. Elective induction at 39 weeks. For low-risk pregnancies with no medical problem, ACOG considers it reasonable to offer induction at or beyond 39 weeks 0 days — the approach validated by the ARRIVE trial and carried into ACOG's current guidance (a 2025 Clinical Practice Update). The key words are "offer" and "39 weeks." It is an option, not a requirement, and elective induction is never done before 39 weeks 0 days, because earlier delivery carries avoidable newborn risks.
The medical reasons labor gets induced
When there's a medical indication, the question shifts from whether to deliver to when. ACOG has published detailed guidance on timing. A few of the most common reasons:
- Going past the due date (late-term and postterm). Risks to the baby rise as a pregnancy stretches beyond 41 weeks. ACOG says induction can be considered between 41 weeks 0 days and 42 weeks 0 days, and is recommended after 42 weeks 0 days (and by 42 weeks 6 days). This is one of the most frequent reasons for induction anywhere.
- High blood pressure conditions (gestational hypertension and preeclampsia). These are a leading reason to deliver early. For gestational hypertension or preeclampsia without severe features, ACOG generally recommends delivery around 37 weeks; with severe features, earlier.
- Gestational diabetes, especially when it requires medication or isn't well controlled.
- The baby measuring small (fetal growth restriction) or low amniotic fluid (oligohydramnios).
- The water breaking before labor starts (prelabor rupture of membranes).
- Intrahepatic cholestasis of pregnancy and several other less common conditions.
An important principle from ACOG ties all of these together: when there is a genuine medical or obstetric indication for earlier delivery, the team should not wait until 39 weeks just for the sake of reaching it. The condition drives the timing.
Why induction comes up so often in surrogacy
Induction is a frequent topic in surrogacy care, even when a pregnancy is progressing normally. Several factors explain why — and most of them are reassuring rather than alarming.
Surrogates are healthy, experienced, and well screened. Following ASRM guidance, a gestational carrier has already had at least one full-term, uncomplicated delivery. Experienced mothers tend to have a more favorable cervix and respond more predictably to induction, which makes the process smoother and keeps the cesarean risk low. The very things that qualify someone to be a surrogate also make an induction, if needed, straightforward.
Pregnancies are watched closely. Surrogacy pregnancies receive attentive prenatal care, and care teams often have a lower threshold to deliver at term rather than let a pregnancy run long.
The way these pregnancies are conceived plays a role. Most surrogacy pregnancies are conceived through a frozen embryo transfer (FET), and many use a "programmed" cycle, in which medication prepares the uterus and no corpus luteum forms. A growing body of research links programmed FET cycles to a modestly higher risk of hypertensive disorders of pregnancy, likely because the corpus luteum normally produces vasoactive hormones (such as relaxin) that help the mother's circulation adapt. Because high blood pressure is itself a common reason to induce, this is one concrete reason the topic comes up. It is also exactly why your team monitors the surrogate's blood pressure carefully — so that if something develops, it's caught early and managed calmly.
Coordination matters — within medical limits. A planned delivery window can help everyone prepare: the surrogate, the clinical team, and intended parents who are often traveling, sometimes from abroad. But this only ever happens inside medically appropriate timing. Logistics never override the medicine — elective timing still respects the 39-week floor, and any earlier delivery happens only for a medical reason.
How an induction actually works
There's no single "induction." The team chooses methods based on how ready the cervix is. Commonly:
- Membrane sweep (stripping): a quick in-office step that can encourage labor to start on its own.
- Cervical ripening: softening and opening the cervix using prostaglandin medication or a small balloon catheter (a Foley/cervical balloon). This is often the first step when the cervix isn't ready.
- Breaking the water (amniotomy): the doctor releases the amniotic fluid once the cervix has opened, which can strengthen labor.
- Oxytocin (Pitocin): an IV medication that produces and regulates contractions. It's the same hormone the body uses naturally, given in a controlled, monitored way.
An induction can take anywhere from several hours to more than a day, particularly for cervical ripening. That's normal. Throughout, the surrogate and baby are monitored, and the team adjusts as labor progresses.
Who actually decides? (The part everyone should be clear on)
This is where surrogacy differs from an ordinary pregnancy, and where expectations need to be set early.
Under the 2023 ASRM Ethics Committee opinion, the gestational carrier is the sole decision-maker regarding her own medical care — through prenatal care, labor, delivery, and recovery. Intended parents cannot require an induction or override a medical decision about the surrogate's body. One practical nuance is worth understanding: when an induction would be elective (no medical indication), intended parents may share a preference — about timing, or about being present — and the team can take it into account if the surrogate agrees and her doctor considers it medically appropriate. When an induction is medically indicated, the timing follows the condition and the obstetrician's judgment. Either way, the final decision belongs to the surrogate, guided by her doctor.
That framework protects everyone:
- For surrogates: your body, your care, your call. No one can schedule or refuse a medical procedure on your behalf. A good agency and a good set of intended parents will respect that completely.
- For intended parents: the most useful thing you can do is trust the medical team and stay flexible. Your role is to be ready and present, not to manage the clinical timeline.
A well-drafted surrogacy agreement reflects this reality. It typically confirms the surrogate's decision-making authority over her care while setting shared expectations about communication, who's present at the birth, and how decisions get communicated — so that when an induction is discussed, no one is surprised.
What this means for intended parents
A few practical takeaways:
- Plan travel with a buffer. Because deliveries — induced or spontaneous — rarely land exactly on the due date, build flexibility into flights and lodging, especially for international intended parents. Your agency's coordinator can help you read the signals as term approaches.
- A planned induction can be reassuring. It usually means the team has a clear plan and monitoring in place — while still keeping medical judgment first.
- Let the medicine lead. The surrogate and her doctor decide the method and timing. Your job is to be there for the moment your baby arrives.
What this means for surrogates
- Induction is routine, and you've likely been through labor before. As an experienced mother, you're in a strong position for a smooth induction if one is recommended.
- You stay in control of your care. Every step is your decision, made with your OB. You can ask questions, request explanations, and decline anything you're not comfortable with.
- Speak up about your blood pressure and how you're feeling. Because programmed FET pregnancies carry a slightly higher chance of high blood pressure, your honest reports help your team keep you safe.
The bottom line
Induction is a normal, well-studied part of American obstetrics, and it's a frequent part of surrogacy care, for reasons that mostly reflect careful, proactive monitoring. It does not signal that something has gone wrong. And in surrogacy, the decision is anchored where it belongs — with the surrogate and her doctor — so that every birth happens safely and on terms everyone has agreed to in advance.
Talk it through with Ivy Surrogacy
At Ivy Surrogacy, a question like this one never gets handed to a call center. Our in-house clinical team — clinicians with nursing and IVF backgrounds — personally reviews medical records and walks both surrogates and intended parents through what to expect at each stage, including delivery. So when your OB raises induction, you already know what it means and why.
Whether you are an intended parent mapping out your journey or a woman considering becoming a surrogate, we would be glad to answer your questions.
Talk with the Ivy Surrogacy team
Frequently Asked Questions
1. Does an induction mean something is wrong with the baby or the surrogate?
Usually not. Many inductions are planned, proactive decisions — including elective induction at 39 weeks in low-risk pregnancies. When there is a medical reason, induction is a way to manage risk safely, not a sign of an emergency.
2. Does being induced make a cesarean more likely?
No. The large ARRIVE trial found that elective induction at 39 weeks did not raise the cesarean rate and slightly lowered it compared with waiting for labor. For experienced mothers, like surrogates, induction tends to be especially predictable.
3. Can intended parents request or schedule an induction?
They can share a preference, but they cannot require it. For an elective induction, intended parents may express a preference — for example, about timing — which the team can consider if the surrogate agrees and it is medically appropriate. For a medically indicated induction, the timing follows the doctor's judgment. Under ASRM's 2023 ethics guidance, the surrogate is the sole decision-maker about her medical care, and the final call is always hers, together with her obstetrician.
4. Can a surrogate refuse an induction?
Yes. A gestational carrier makes her own medical decisions together with her obstetrician. If an induction is recommended, her doctor should explain the reason, the benefits, the risks, and any alternatives, and the decision is hers.
5. Why does induction come up so often in surrogacy?
A few reasons: surrogates are healthy, experienced mothers who tend to respond well to induction; these pregnancies are monitored closely; and programmed frozen embryo transfer cycles — common in surrogacy — carry a modestly higher risk of high blood pressure conditions that can call for delivery.
6. When is labor induced for going past the due date?
ACOG considers induction reasonable between 41 weeks 0 days and 42 weeks 0 days, and recommends it after 42 weeks 0 days (by 42 weeks 6 days), because risks to the baby rise the longer a pregnancy continues past term.
7. How long does an induction take?
It varies. Preparing the cervix can take several hours to more than a day, after which labor proceeds. The surrogate and baby are monitored throughout, and the team adjusts as things progress.
8. Can intended parents be present during the induction and birth?
Often yes, but it depends on the hospital's policy, the birth plan, and the surrogate's consent. It is best to discuss expectations — who will be in the room, and when — well before delivery.
Sources
- CDC / NCHS. Induction of Labor Increases in the United States: 2016 to 2024. Data Brief No. 554, 2026. https://www.cdc.gov/nchs/products/databriefs/db554.htm
- Grobman WA, et al. Labor Induction versus Expectant Management in Low-Risk Nulliparous Women (the ARRIVE trial). N Engl J Med, 2018. https://pubmed.ncbi.nlm.nih.gov/30089070/
- ACOG. Management of Full-Term Nulliparous Individuals Without a Medical Indication for Delivery (Clinical Practice Update), 2025. https://pubmed.ncbi.nlm.nih.gov/39513607/
- ACOG. Management of Late-Term and Postterm Pregnancies (Practice Bulletin No. 146), 2014. https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2014/08/management-of-late-term-and-postterm-pregnancies
- ACOG. Medically Indicated Late-Preterm and Early-Term Deliveries (Committee Opinion No. 831), 2021. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2021/07/medically-indicated-late-preterm-and-early-term-deliveries
- ACOG. Cervical Ripening in Pregnancy (Clinical Practice Guideline), 2025. https://journals.lww.com/greenjournal/fulltext/2025/07000/cervical_ripening_in_pregnancy__acog_clinical.30.aspx
- ACOG. When Pregnancy Goes Past Your Due Date (patient FAQ). https://www.acog.org/womens-health/faqs/when-pregnancy-goes-past-your-due-date
- ASRM. Recommendations for Practices Using Gestational Carriers (committee opinion), 2022. https://www.asrm.org/practice-guidance/practice-committee-documents/recommendations-for-practices-using-gestational-carriers-a-committee-opinion-2022/
- ASRM. Consideration of the Gestational Carrier (Ethics Committee opinion), 2023. https://www.asrm.org/practice-guidance/ethics-opinions/consideration-of-the-gestational-carrier-an-ethics-committee-opinion-2023/
- Programmed Frozen Embryo Transfer and Hypertensive Disorders of Pregnancy. Fertil Steril, 2022. https://www.fertstert.org/article/S0015-0282(22)00484-8/fulltext
- Wang Z, et al. Increased Risk of Pre-eclampsia After Frozen-Thawed Embryo Transfer in Programming Cycles. Front Med, 2020. https://pmc.ncbi.nlm.nih.gov/articles/PMC7156607/



