As an intended parent, you may come across intrahepatic cholestasis of pregnancy — usually shortened to ICP — in one of two ways. A surrogate you are considering may have had it in an earlier pregnancy, and you have to decide what that means for matching. Or a surrogate already carrying your baby may be diagnosed with it partway through the journey. Either way, the name alone can be unsettling.
So it is worth saying plainly, up front: ICP is one of the most common and best-understood conditions that occur only in pregnancy. It carries low long-term risk for the surrogate herself, and it is managed along a clear, evidence-based path that obstetricians follow every day. This article walks through what ICP actually is, where the real risks lie, how a past history factors into matching, and what to expect if it is diagnosed during the pregnancy.
What is intrahepatic cholestasis of pregnancy (ICP)?
ICP is the most common liver condition specific to pregnancy. It typically appears in the second or third trimester, when pregnancy hormones temporarily slow the normal flow of bile, allowing bile acids to build up in the bloodstream.
Its hallmark is itching without a rash — often most noticeable on the palms of the hands and the soles of the feet, and frequently worse at night. Itching is common in pregnancy for ordinary reasons, so ICP is confirmed not by the symptom alone but by a blood test that measures serum total bile acids, usually alongside liver function. Diagnostic cutoffs vary by lab and guideline; many U.S. practices use a total bile acid level above 10 µmol/L, while the data behind that exact threshold are acknowledged to be limited. In the United States, ICP affects roughly 0.8 to 1 percent of pregnancies, with higher rates in some populations.
Is ICP dangerous for the surrogate?
For the surrogate, ICP usually carries low long-term risk — but "low risk" is not the same as "nothing to manage." The main burden is the itching itself, which can be intense enough to disturb sleep and daily life. Some people also have raised liver enzymes, and before settling on the diagnosis the care team runs tests to rule out other liver and bile-duct conditions. So ICP is taken seriously and followed medically.
The reassuring part still holds: once the baby is delivered, the surrogate's symptoms typically ease within a few weeks, and follow-up blood tests confirm that liver values and bile acids have returned to normal. For the pregnant person, ICP is not known to cause lasting harm.
What are the risks to the baby?
The reason ICP is monitored so closely is its potential effect on the baby — primarily a higher chance of preterm birth and of meconium in the amniotic fluid, and, in more severe cases, an increase in the risk of a serious adverse outcome late in pregnancy. The entire approach to ICP — closer monitoring, then a planned, well-timed delivery — exists specifically to stay ahead of that risk.
Here is where the evidence is genuinely reassuring. Large studies — including a 2019 analysis that both U.S. and U.K. guidelines rely on — found that the increased risk of the most serious outcome is concentrated in the severe group: surrogates with bile acids at or above 100 µmol/L. Below that level, and without other complications, the risk stays close to the background rate of any pregnancy.
Bile acid levels and ICP severity
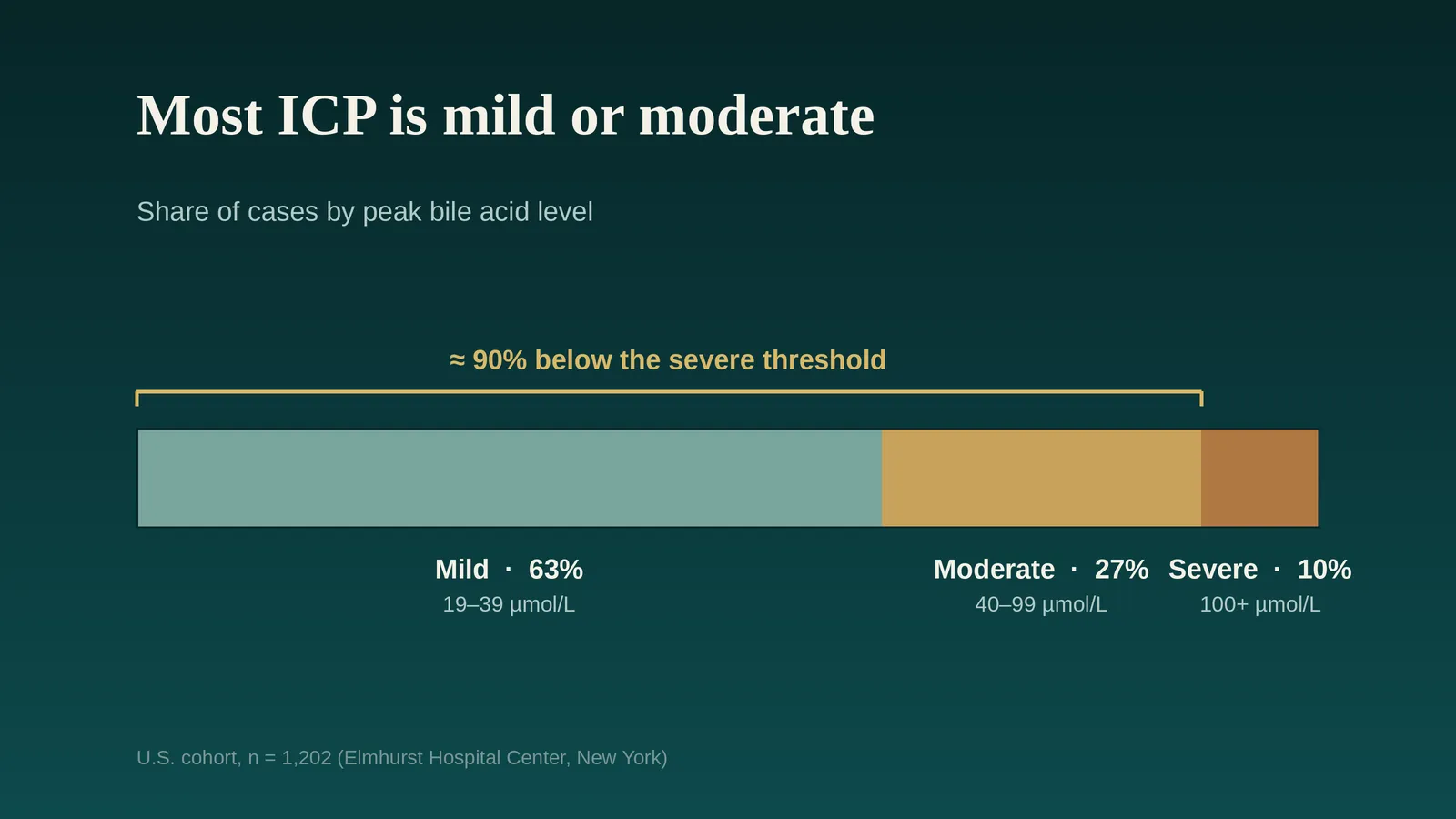
Because risk tracks so closely with one number, clinicians think about ICP in bands based on the highest (peak) bile acid level. The U.K. RCOG guideline defines them as mild (19–39 µmol/L), moderate (40–99 µmol/L), and severe (100 µmol/L or above). U.S. guidance from the Society for Maternal-Fetal Medicine works mainly off a simpler split — below 100 versus 100 or above — for decisions about delivery timing.
Peak bile acids | Common interpretation | Share of ICP cases | What it may mean for care |
|---|---|---|---|
19–39 µmol/L | Mild | Most cases — about 63% fall below 40 µmol/L | Monitoring and symptom relief; delivery timing individualized, often toward the later end of the guideline window |
40–99 µmol/L | Moderate | About 27% | Closer attention; planned delivery often earlier within the guideline window |
100 µmol/L or above | Severe (highest-risk group) | A minority — about 10% | In U.S. guidance, planned delivery commonly offered around 36 weeks |
Proportions are based on a U.S. cohort of 1,202 pregnancies (Elmhurst Hospital Center, New York). Exact figures vary by population — severe ICP is more common in some groups than others — but across studies the great majority of cases fall below the severe threshold. Labels and cutoffs vary by guideline and lab; this is a general guide, not a treatment rule, and the care team decides based on the full picture.
This is one of the most reassuring facts about ICP, and it is worth stating plainly: in this U.S. cohort, about 90% of cases fell below the severe threshold, and severe ICP was a minority. That is why care can be matched to the actual numbers rather than treating every case as a worst case.
Can a surrogate with a history of ICP be matched?
A past episode of ICP is the strongest single predictor of having it again, so it is reasonable to factor it into a matching decision. But the recurrence figure is often misread. Across the literature it runs roughly 40 to 60 percent, with a recent, more diverse cohort landing near 44 percent.
Read that the other way around, which is the honest way to read it: in a large share of pregnancies, ICP does not come back at all. A prior episode is a flag to watch, not a verdict. It is entirely common for a surrogate with a history of ICP to carry a pregnancy in which it never reappears.
A history of ICP, by itself, does not rule a surrogate out. It is a known and manageable factor, and evaluating it well means looking at the specifics rather than the label alone. If you are weighing such a match, these are the questions a careful evaluation considers:
- What was her highest (peak) bile acid level in the affected pregnancy? (Levels above 40 are linked to a higher chance of recurrence.)
- At what point in pregnancy did ICP appear?
- Did her symptoms and lab values resolve after delivery?
- Was delivery moved earlier because of ICP?
- Were there any complications for the baby or newborn?
- Is the planned journey a singleton or a multiples pregnancy? (Multiples carry a higher baseline rate.)
With those answers, you and the care team can evaluate the situation on its specifics rather than make a reflexive yes or no. For most healthy candidates, a well-managed history of mild-to-moderate ICP is compatible with a successful surrogacy.
What happens if a surrogate is diagnosed with ICP?
It helps to know that ICP very often appears for the first time in a pregnancy, with no prior history at all. So this is not a situation reserved for surrogates who were flagged in advance — it can simply arise, and the care team is well prepared for it when it does. If your surrogate is diagnosed, here is what typically follows.
Monitoring steps up. Bile acids and liver function are tracked, and the pregnancy moves to a closer surveillance schedule.
Treatment focuses on comfort. The standard first-line medication is ursodeoxycholic acid (UDCA). It is used mainly to treat the surrogate's symptoms and may ease itching for some people, although the largest trial to date (PITCHES) did not show a clear improvement in outcomes for the baby. It remains the usual first choice for symptom relief.
The baby is watched more closely. This may include non-stress tests or biophysical profiles, generally starting at the point in pregnancy when the team would act on an abnormal result — or at diagnosis, if ICP is found later.
Delivery is planned, and the timing is the central decision. Because the late-pregnancy risk concentrates near term and rises with higher bile acid levels, obstetricians plan delivery rather than waiting for the due date. Current U.S. guidance ties the window to the highest bile acid value recorded during the pregnancy:
- Bile acids below 100 µmol/L — delivery between 36 and 39 weeks
- Bile acids 100 µmol/L or above — delivery offered at 36 weeks
- Complicated cases (severe persistent symptoms, certain prior history, or other liver disease) — sometimes 34 to 36 weeks
This is why a surrogacy affected by ICP often ends with a planned induction a few weeks before the due date. It is not a sign that something has gone wrong — it is the deliberate, evidence-based step that keeps a small risk small.
Your role as an intended parent is mostly to stay informed and stay in step with the care team: understand why the timeline may move up, and trust that the plan is built around the numbers.
Questions intended parents often ask
1. Is the surrogate herself in danger?
Usually not in the long term. ICP's main burden for the surrogate is itching, which can be significant, and it calls for medical follow-up — but it typically resolves after delivery and is not known to cause lasting harm to the pregnant person.
2. Can a surrogate with a history of ICP be matched?
Often, yes. A history is a manageable factor, not an automatic disqualifier, and many such pregnancies are entirely unaffected. The right call depends on the specifics of the earlier episode and the candidate's overall health.
3. Does a diagnosis mean something is wrong with the baby?
No. A diagnosis means the pregnancy moves to closer monitoring and a planned delivery window — steps designed to prevent problems, not signs that one has occurred.
4. Why deliver early?
Because the small late-pregnancy risk is concentrated near term and in higher-bile-acid cases. Delivering within the recommended window is how that risk is avoided.
5. Will it have lasting effects?
For the surrogate, no — it resolves after delivery, confirmed by follow-up labs. (A history does raise the odds of ICP in a future pregnancy, which is the link back to the matching question above.)
The bottom line
ICP can sound frightening, especially when it touches a pregnancy you have waited a long time for. But it is common, well-characterized, and managed along a path obstetricians know well: confirm it with a blood test, monitor closely, relieve the symptoms, and plan a well-timed delivery. The long-term risk to the surrogate is low, most cases sit below the highest-risk band, and the outcome that gets the most attention is precisely the one the whole plan is designed to prevent.
Whether you are weighing a match or navigating a diagnosis, the goal is the same: to make decisions from clear information rather than from worry. The questions above are a good place to start that conversation with your care team.
This article is for educational purposes and does not replace medical advice from the surrogate's obstetrician or maternal-fetal medicine specialist.
References
- Society for Maternal-Fetal Medicine; Lee RH, Greenberg M, Metz TD, Pettker CM. SMFM Consult Series #53: Intrahepatic Cholestasis of Pregnancy. American Journal of Obstetrics & Gynecology. 2021;224(2):B2–B9.
- StatPearls. Pregnancy Intrahepatic Cholestasis. NCBI Bookshelf.
- American College of Obstetricians and Gynecologists. Committee Opinion No. 831: Medically Indicated Late-Preterm and Early-Term Deliveries. Obstetrics & Gynecology. 2021;138(1):e35–e39.
- Girling J, Knight CL, Chappell L. Intrahepatic Cholestasis of Pregnancy (Green-top Guideline No. 43). BJOG. 2022;129(13):e95–e114.
- Ovadia C, Seed PT, Sklavounos A, et al. Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: results of aggregate and individual patient data meta-analyses. The Lancet. 2019;393(10174):899–909.
- Chappell LC, Bell JL, Smith A, et al. Ursodeoxycholic acid versus placebo in women with intrahepatic cholestasis of pregnancy (PITCHES): a randomised controlled trial. The Lancet. 2019;394(10201):849–860.
- Sarker M, Ramirez Zamudio A, DeBolt C, Ferrara L. Beyond stillbirth: association of intrahepatic cholestasis of pregnancy severity and adverse outcomes. American Journal of Obstetrics & Gynecology. 2022;227(3):517.e1–517.e7.
- Rosenberg HM, Sarker MR, Ramos GA, Bianco A, Ferrara L, DeBolt CA. Intrahepatic Cholestasis of Pregnancy Recurrence in a Subsequent Pregnancy. Obstetrics & Gynecology. 2026;147(2):239–241.



