Key Takeaways
- Purpose: PGT-M helps families with a known single-gene mutation reduce the risk of passing it to their child.
- Who Needs It: Recommended when both partners are carriers of the same recessive condition, one partner has a dominant condition, or for X-linked disorders.
- Process: Requires IVF, embryo biopsy, customized genetic analysis, and is always followed by a recommendation for prenatal confirmation.
- Scope: PGT-M is for single-gene disorders. It is not designed for complex, polygenic conditions like diabetes or most cancers, although exceptions exist for some hereditary cancer syndromes.
- Cost in the U.S.: $7,000–$12,000 for PGT-M (in addition to IVF, medication, and transfer costs).
- Timeline: Test development 3–8 weeks, results in ~2–3 weeks; the overall process typically takes 6–12 weeks.
- Alternatives: Choosing a donor with genetic screening may avoid the need, but couples who both carry the same variant usually require it.
- Prenatal Care: Even after PGT-M, ASRM and ACOG recommend confirmation with CVS or amniocentesis.
What Is PGT-M?
Preimplantation Genetic Testing for Monogenic conditions (PGT-M) is a laboratory procedure that allows intended parents undergoing IVF to test embryos for a specific, known single-gene mutation before transfer. This targeted testing makes it possible to select embryos unaffected by the condition, significantly lowering the chance of transmitting serious inherited diseases.
A Brief History of PGT-M
- 1990s: Early attempts, then called preimplantation genetic diagnosis (PGD), relied on day-3 blastomere biopsy and PCR of a single cell. This was groundbreaking but limited by technical challenges like allele drop-out (where one of the two gene copies in a cell fails to be detected), which could lead to misdiagnosis.
- 2000s–2010s: The field advanced to day-5/6 trophectoderm biopsy (removing 5–10 cells). This, combined with whole-genome amplification and advanced haplotype analysis (which tracks the genetic neighborhood around the mutation), significantly improved both accuracy and embryo safety.
- Today: U.S. labs widely use next-generation sequencing (NGS) methods combining direct mutation analysis with informative family-specific markers. Current guidance from ASRM and ACOG outlines when PGT-M is appropriate, emphasizes residual risk, and recommends prenatal confirmation.
Who Should Consider PGT-M?
PGT-M is recommended when there is a clear, documented genetic risk in the family:
- Autosomal dominant disorders: When one parent carries or is affected by a dominant mutation (e.g., Huntington disease, Marfan syndrome).
- X-linked conditions: When there is a known family mutation causing disorders such as Duchenne muscular dystrophy.
- Autosomal recessive conditions: When both partners are carriers of the same mutation, or they already have an affected child.
- Special use cases: HLA matching (to help a sibling with stem cell therapy), and some mitochondrial DNA conditions (handled in highly specialized centers).
👉 A Note on Different PGT Types: PGT-M focuses on single-gene mutations. For families dealing with chromosomal issues like translocations, a different test called PGT-SR is used. We’ll explore this more in the comparison section below.
The PGT-M Process Step by Step
Genetic Counseling and Family Work-up
- Confirm the precise familial mutation. A confirmed pathogenic (disease-causing) variant is required.
- Understanding VUS: Sometimes, a “variant of uncertain significance” (VUS) is found. This is a genetic change where science doesn’t yet have enough evidence to know if it’s harmless or disease-causing. Because of this uncertainty, PGT-M cannot be performed for a VUS, as it could lead to discarding a healthy embryo or transferring an affected one. A genetic counselor can explain your family’s specific situation.
- Collect DNA samples from parents (and sometimes relatives) to establish informative markers.
- Provide counseling on limitations and explain that prenatal confirmation is still required.
IVF with ICSI
- The IVF cycle proceeds with ovarian stimulation and egg retrieval.
- Fertilization is usually performed with ICSI (intracytoplasmic sperm injection) to avoid DNA contamination from sperm cells.
- Embryos are cultured to the blastocyst stage (day 5 or 6).
Embryo Biopsy and Freezing
- Several trophectoderm cells are removed from each blastocyst.
- Embryos are vitrified (frozen) while testing is completed.
Laboratory Testing
- NGS is used for direct mutation analysis.
- Linked-marker haplotype testing reduces risks of allele drop-out or recombination errors.
- Some labs can combine PGT-M with PGT-A on the same biopsy sample.
Results and Embryo Selection
Embryos are classified as:
- Affected (carry both mutations for a recessive condition or the dominant mutation).
- Carrier (one copy of a recessive mutation).
- Unaffected/Non-carrier. Unaffected embryos are prioritized for transfer.
Illustration: Example of a combined PGT-M + PGT-A report
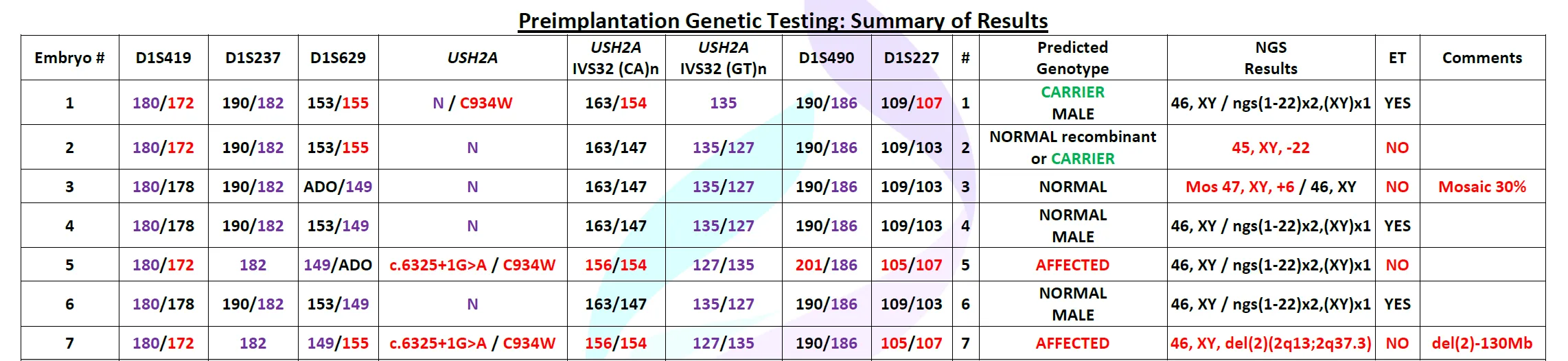
The report below shows how laboratories integrate single-gene testing (PGT-M) with chromosomal screening (PGT-A):
- Left columns: STR markers and the family’s known USH2A mutation confirm whether embryos are normal, carriers, or affected.
- Middle section: Each embryo is labeled as Normal, Carrier, or Affected.
- Right columns: PGT-A results indicate whether the embryo is chromosomally normal (euploid), abnormal (aneuploid), or mosaic.
- ET column: Lists which embryos are considered suitable for transfer.
👉 In this example, embryos #4 and #6 are normal and euploid, while #1 (a carrier, but unaffected) is also considered suitable for transfer. Embryos with aneuploidy, mosaicism, or affected status are excluded.
Prenatal Confirmation
- Even when PGT-M results are reassuring, ASRM and ACOG recommend prenatal diagnostic confirmation through CVS or amniocentesis.
Cost of PGT-M in the U.S.
PGT-M costs vary depending on clinic and laboratory contracts, but most intended parents can expect:
- IVF with ICSI: $14,000–$20,000
- Fertility medications: $3,500–$8,000
- PGT-M testing (including biopsy and lab analysis): $7,000–$12,000 per cycle, or $350–$500 per embryo
- Frozen embryo transfer (FET): $3,000–$5,000
💡 At Ivy Surrogacy, we provide transparent cost guidance and connect you with trusted clinics and labs so there are no financial surprises.
How Long Does PGT-M Take?
- Family-specific assay development: Typically 3–8 weeks for the first cycle.
- Lab analysis after biopsy: 2–3 weeks (sometimes faster for established families).
- Overall process: From genetic work-up through embryo transfer, expect 6–12 weeks.
Advantages of PGT-M
- Prevents passing on known single-gene disorders.
- Avoids emotionally difficult choices after prenatal diagnosis.
- Applicable to most monogenic diseases once the mutation is identified.
- Enables specialized uses such as HLA matching.
- Reduces uncertainty for families with a strong genetic history.
Limitations of PGT-M
- Requires a confirmed pathogenic variant; VUS cannot be reliably tested.
- Residual risk remains from recombination, mosaicism, or lab error.
- IVF is necessary, with its medical and emotional demands.
- Not every cycle yields embryos that are genetically suitable and viable.
- Raises ethical considerations for late-onset conditions like Huntington’s disease or BRCA-related cancers.
Can PGT Screen for Complex Conditions Like Cancer or Diabetes?
This is a common and important question. For most common diseases, the answer is no, but there are key exceptions.
- Single-Gene vs. Multifactorial Conditions: PGT-M is designed for single-gene conditions, where one specific mutation directly causes a disease. Most common health issues—like hypertension, type 2 diabetes, psychiatric disorders, and most cancers—are multifactorial. They result from a complex interplay between hundreds of genes (polygenic) and environmental factors. Standard PGT cannot screen for these complex conditions.
- The Exception – Hereditary Cancer Syndromes: Some families have a high cancer risk due to a single-gene mutation, such as BRCA1/BRCA2. In these specific cases, PGT-M can be used to select embryos that have not inherited this high-risk mutation.
- Emerging Technology (PGT-P): A new, still controversial test called PGT-P (for Polygenic conditions) attempts to calculate a “risk score” for embryos. This is not yet standard of care and its clinical benefit is still debated.
If you have a family history of these conditions, a genetic counselor can provide the best guidance.
PGT-M vs. PGT-A vs. PGT-SR
Although they all involve embryo testing, these tests answer different questions:
- PGT-M (Monogenic): Detects whether an embryo carries a specific, known single-gene mutation in your family.
- PGT-A (Aneuploidy): Screens embryos for the wrong number of chromosomes (e.g., trisomy 21), which can lead to failed implantation, miscarriage, or conditions like Down syndrome.
- PGT-SR (Structural Rearrangements): Used when a parent has a known chromosomal rearrangement, like a translocation, to find embryos with the correct amount of chromosomal material.
👉 For more details, see our article on PGT-A.
FAQs About PGT-M
1. What is the accuracy of PGT-M?
PGT-M is highly accurate (>95%) for detecting known familial mutations. However, the exact rate can vary depending on the specific gene and lab. This residual risk is why confirmatory prenatal testing is always recommended.
2. Does PGT-M harm embryos?
Modern trophectoderm biopsy has a minimal impact on embryo viability, and U.S. clinics report excellent success rates after biopsy.
3. Is PGT-M covered by insurance?
Coverage varies widely. Some U.S. insurance plans cover PGT-M when there is a clear medical indication; others may not. Always check with your provider.
4. Can PGT screen for conditions like diabetes or a family history of cancer?
Generally, no. PGT-M is for single-gene diseases. Most common conditions like diabetes or hypertension are too genetically complex. The main exception is hereditary cancer syndromes caused by a single gene (like BRCA), for which PGT-M can be used.
5. How long does the process take from start to embryo transfer?
From genetic setup through results and frozen embryo transfer, the process usually takes 6–12 weeks.
6. Can PGT-M test for multiple conditions at once?
Yes, some labs can design assays to test for more than one familial condition, but this increases complexity and cost.
7. What if no healthy embryos are found?
Options include repeating IVF, using donor sperm or eggs, or considering adoption, depending on family goals.
8. Can PGT-M and PGT-A be done together?
Yes, both tests can be performed on the same biopsy. Many families choose this option to check for both genetic mutations and chromosomal abnormalities.
Ready to Take the Next Step?
At Ivy Surrogacy, we understand how overwhelming genetic risks can feel. Our experienced team works closely with top fertility clinics and genetic counselors to design the safest, most effective path for your family.
Whether you’re considering PGT-M, PGT-A, or donor options, we’ll guide you through every stage with clarity, compassion, and expertise.
👉 Contact us today to schedule a free consultation and learn how Ivy Surrogacy can support your journey toward a healthy pregnancy.



