Choosing an egg donor is not only about age, appearance, education, or family background. For intended parents, one of the most important questions is medical:
Is this donor likely to produce enough mature eggs in one cycle to give us a strong chance of creating healthy embryos?
That is where two ovarian reserve markers become especially important: AMH and AFC.
AMH and AFC do not tell us everything. They do not directly measure egg quality, and they do not guarantee embryo success. But they are among the most useful tools fertility physicians use to estimate how a donor may respond to ovarian stimulation.
For intended parents investing significant time, money, and emotion into an egg donation cycle, understanding these numbers can help you ask better questions, avoid preventable risk, and make more confident decisions.
Quick Answer
A qualified egg donor is usually young, healthy, medically screened, genetically screened, psychologically evaluated, and expected to respond well to ovarian stimulation.
Two key ovarian reserve markers used during donor evaluation are:
- AMH, a blood test that reflects ovarian reserve.
- AFC, an ultrasound count of small resting follicles in the ovaries.
Many fertility clinics prefer egg donor candidates to have an AMH around 2.0 ng/mL or higher and a combined AFC around 16 or higher, with stronger numbers often suggesting a better expected response. However, these are not universal national cutoffs. Each clinic interprets AMH and AFC together with the donor’s age, ultrasound findings, medical history, prior cycle history, and physician judgment.
Most importantly: AMH and AFC help predict egg quantity, not egg quality. Egg quality is still strongly related to age.
A Real Case: When a Healthy Donor Candidate Did Not Meet the Medical Bar
A first-time egg donor candidate recently completed her baseline ovarian reserve evaluation at a U.S. fertility clinic. Her results were:
- AMH: 1.4 ng/mL
- AFC: 15
On paper, she looked like a strong candidate. She was young, healthy, and had no concerning medical history. But after reviewing her ovarian reserve results, the reproductive endocrinologist felt that her expected response to stimulation might be lower than the clinic’s preferred standard for an egg donor cycle.
The match did not proceed.
This does not mean the donor was unhealthy. It does not mean she could never have children. It simply means that, for the purpose of egg donation, her expected egg yield may not have provided the level of confidence intended parents and fertility physicians typically want before moving forward.
Egg donor standards are often higher than general fertility standards because the goal is different.
For a patient trying to conceive with her own eggs, the question may be:
Can we still attempt treatment?
For an egg donor cycle, the question is:
Is this donor likely to produce enough mature eggs in one retrieval to justify the intended parents’ investment and give them a strong chance of creating usable embryos?
Those are very different standards.
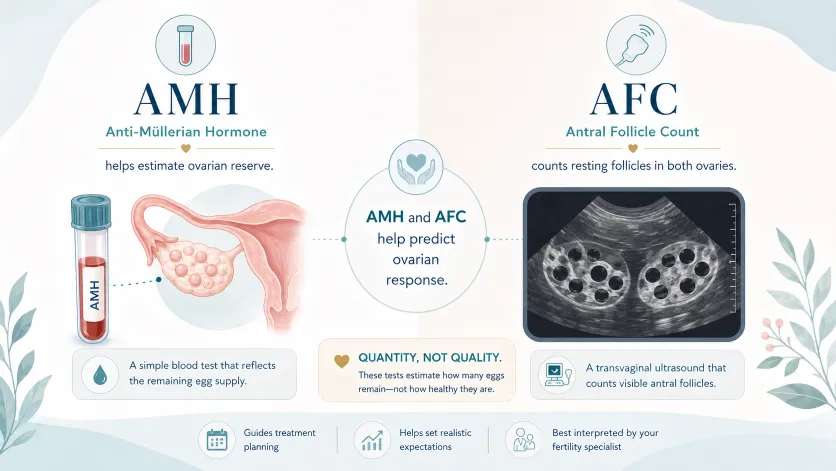
What Are AMH and AFC?
AMH: Anti-Müllerian Hormone
AMH is a blood test that helps estimate ovarian reserve. It reflects the pool of small growing follicles in the ovaries.
One reason AMH is useful is that it is relatively stable throughout the menstrual cycle, so it can often be tested on different cycle days. However, AMH can still be affected by factors such as lab variation and hormonal contraceptive use.
ASRM notes that AMH and AFC are among the simplest and most sensitive markers of ovarian reserve, but they should be interpreted carefully and in context.
AFC: Antral Follicle Count
AFC stands for antral follicle count. It is measured by transvaginal ultrasound, usually early in the menstrual cycle.
During the ultrasound, the physician counts the small follicles, typically around 2–10 mm, in both ovaries. The combined number helps estimate how many follicles may respond during ovarian stimulation.
AFC is especially useful because it gives the physician a direct visual picture of the ovaries before the cycle begins.
Why AMH and AFC Matter in Egg Donation
In egg donation, AMH and AFC are not minor details. They help predict how many eggs may be retrieved during a stimulation cycle.
This matters because IVF is a funnel. Not every follicle produces an egg. Not every egg is mature. Not every mature egg fertilizes. Not every fertilized egg becomes a blastocyst. Not every blastocyst is chromosomally normal.
A strong donor cycle may start with enough follicles to give intended parents multiple chances downstream.
A lower-response cycle may still succeed, but it starts the funnel with fewer opportunities.
That is why fertility physicians pay close attention to ovarian reserve before allowing a donor match to proceed.
Practical Benchmarks Many Clinics Consider
There is no single national AMH or AFC cutoff that every U.S. fertility clinic uses. ASRM’s 2024 guidance on gamete and embryo donation outlines broad donor evaluation recommendations, but it does not establish one universal AMH or AFC threshold for all egg donor candidates.
In clinical practice, however, many programs use preferred ranges to help assess whether a donor is likely to respond well.
A practical framework may look like this:
Marker | Commonly Preferred Minimum | Stronger / More Reassuring Range | Why It Matters |
|---|---|---|---|
AMH | Around 2.0 ng/mL or higher | Around 3.0 ng/mL or higher | Helps estimate expected ovarian response |
AFC | Around 16 or higher, both ovaries combined | Around 20 or higher | Helps estimate the number of follicles likely to respond |
These numbers should not be treated as absolute rules. A physician may consider a donor differently depending on age, prior retrieval history, AFC pattern, body weight, medication protocol, and whether the donor has recently used hormonal contraception.
But for intended parents, these benchmarks are useful because they help identify whether a donor is likely to produce a strong number of mature eggs in a single cycle.
Reading the Case Through This Framework
In the case above, the donor had:
Marker | Donor’s Result | Practical Benchmark | Interpretation |
|---|---|---|---|
AMH | 1.4 ng/mL | Often preferred around ≥2.0 ng/mL | Lower than many programs prefer |
AFC | 15 | Often preferred around ≥16 | Borderline low |
Neither number, by itself, proves that the donor could not produce healthy eggs. However, both numbers together suggested a potentially lower response.
For intended parents, this matters because a low-response donor cycle may produce fewer mature eggs, fewer blastocysts, and fewer embryos available for transfer or future family building.
The physician’s decision was not about judging the donor as a person. It was about protecting the intended parents from taking avoidable risk at the very beginning of the process.
AMH and AFC Predict Quantity, Not Quality
One of the most important points to understand is this:
AMH and AFC predict egg quantity more than egg quality.
ASRM’s ovarian reserve guidance states that ovarian reserve markers are useful for predicting oocyte yield after controlled ovarian stimulation, but they are poor independent predictors of reproductive potential.
In other words, AMH and AFC can help answer:
How many eggs might we retrieve?
They do not reliably answer:
Will those eggs create healthy embryos?
Egg quality is more strongly related to age. This is why egg donors are usually young, often in their 20s. A young donor with lower AMH may still have good egg quality, but she may produce fewer eggs.
For intended parents, the issue is not whether success is possible. The issue is whether the cycle provides enough probability and enough margin.
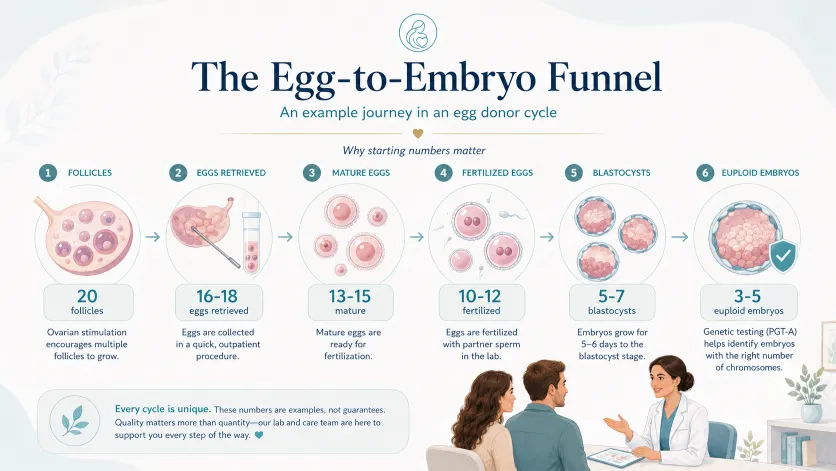
The Egg-to-Embryo Funnel
A donor with strong ovarian reserve may produce a cycle that looks roughly like this:
- 20 follicles
- 16–18 eggs retrieved
- 13–15 mature eggs
- 10–12 fertilized eggs
- 5–7 blastocysts
- 3–5 chromosomally normal embryos, depending on age and lab factors
A donor with lower ovarian reserve might produce a smaller funnel:
- 12–15 follicles
- 8–12 eggs retrieved
- 6–10 mature eggs
- 5–8 fertilized eggs
- 2–4 blastocysts
- 1–3 chromosomally normal embryos
These are not guarantees. Every cycle is different. Some lower-reserve donors may perform better than expected, and some high-reserve donors may perform worse than expected.
But in IVF, starting with fewer eggs usually means fewer opportunities at each step.
This is why intended parents should pay attention to AMH and AFC before committing to a donor cycle.
Why Donor Standards Are Higher Than General Fertility Standards
A woman with AMH of 1.4 ng/mL may still be able to conceive naturally or through fertility treatment. A lower AMH result does not automatically mean infertility.
But egg donation is different.
The goal is not simply to prove that the donor has reproductive potential. The goal is to produce enough mature eggs in one retrieval to give another family a strong chance of creating embryos.
That is why fertility clinics may apply stricter expectations to egg donors than they would to patients using their own eggs.
For intended parents, this distinction is important. A donor can be healthy and still not be the best choice for a donor cycle.
What Intended Parents Should Ask Before Proceeding
If a donor’s AMH or AFC is lower than the clinic’s preferred range, intended parents should not panic. But they should ask direct questions before moving forward.
Useful questions include:
- What egg yield does the physician realistically expect from this donor?
- Is the donor’s AFC consistent with her AMH?
- Could hormonal contraception be making the numbers look lower than they really are?
- Would repeat testing be helpful?
- How many mature eggs would the clinic consider an acceptable outcome?
- If the cycle produces a low number of eggs, what are our options?
- Would the agency support a rematch based on these medical findings?
A reputable agency should welcome these questions. Intended parents deserve to understand the medical reasoning behind a match before committing financially and emotionally.
When a Rematch Discussion Makes Sense
A rematch may be reasonable when:
- AMH is clearly below the clinic’s preferred range.
- AFC is clearly below the clinic’s preferred range.
- Both AMH and AFC suggest a lower expected response.
- The donor has no prior successful retrieval history.
- The intended parents want multiple children from one donor cycle.
- The intended parents are international and have limited travel or timeline flexibility.
- The physician expresses concern about expected egg yield.
A rematch does not mean the donor is “bad.” It means the match may not be medically or financially optimal for the intended parents’ goals.
For intended parents, the cost difference can be significant. A rematch may delay the process by several weeks. But a low-yield egg retrieval can lead to full IVF costs, fewer embryos, difficult decisions, and possibly another donor cycle later.
In many cases, it is better to address the risk before the cycle begins.
What Prospective Egg Donors Should Know
If you are applying to become an egg donor and your AMH or AFC is lower than expected, it can feel discouraging. But a lower result does not mean you failed.
It means you received valuable information about your own ovarian reserve.
Most women do not learn their AMH or AFC until much later, often after they begin trying to conceive. As a donor candidate, you may receive this information earlier, which can help you make informed decisions about your own reproductive future.
If your numbers are lower than expected, consider these next steps:
1. Speak with a Reproductive Endocrinologist
A single AMH or AFC result should be interpreted in context. Your age, medical history, menstrual cycle, ultrasound findings, and medication history all matter.
2. Ask Whether Hormonal Birth Control Could Be Affecting the Result
Hormonal contraception may lower ovarian reserve markers in some patients, and ASRM notes that these markers may improve after stopping hormonal contraception for some people, especially those with low AFC.
This does not mean everyone should stop birth control before testing. It means your physician should interpret the results carefully.
3. Think About Your Own Family-Building Timeline
If having biological children is important to you, a lower ovarian reserve result may be a reason to think more seriously about timing.
4. Consider Fertility Preservation
Egg freezing or embryo freezing may be worth discussing with a fertility specialist, especially if your ovarian reserve is lower than expected for your age.
A donor screening result may close one donation opportunity, but it can also give you useful information for your own future.
Why Experienced Egg Donors Often Receive Higher Compensation
First-time egg donors are evaluated based on predictions.
Their AMH, AFC, age, health history, and genetic screening can help estimate how they may respond. But until they complete a retrieval cycle, no one knows exactly how many mature eggs they will produce, how many will fertilize, or how many embryos may develop.
Experienced egg donors are different.
They may have documented results from prior cycles, including:
- Number of eggs retrieved
- Number of mature eggs
- Fertilization rate
- Blastocyst development
- Embryo quality
- Whether embryos led to pregnancy or birth
This history reduces uncertainty for intended parents.
That is one major reason experienced donors often receive higher compensation. The higher fee is not only about experience. It is about predictability.
In fertility treatment, predictability has value.
Final Takeaway
AMH and AFC are not the whole story, but they are an important part of egg donor evaluation.
For intended parents, these numbers help estimate whether a donor is likely to produce enough mature eggs in one cycle. For donor candidates, these numbers provide meaningful insight into ovarian reserve and future fertility planning.
The most important point is balance:
AMH and AFC should not be treated as absolute measures of fertility or egg quality. But in egg donation, they are highly relevant because they help predict expected egg yield.
A strong donor match should be emotionally appealing, medically sound, and financially responsible.
When AMH and AFC raise concerns, asking for more medical clarity — and sometimes discussing a rematch — is not being difficult. It is being careful.
Frequently Asked Questions
1. What is a good AMH level for an egg donor?
Many fertility clinics prefer egg donor candidates to have an AMH around 2.0 ng/mL or higher, with 3.0 ng/mL or higher often considered more reassuring. However, AMH is not interpreted alone. Physicians also consider AFC, age, ultrasound findings, medical history, and prior cycle results.
2. What is a good AFC for egg donation?
Many clinics prefer a combined AFC of around 16 or higher, with 20 or higher often suggesting a stronger expected ovarian response. AFC is measured by ultrasound and helps estimate how many follicles may respond during stimulation.
3. Can someone with low AMH still donate eggs?
Sometimes, but it depends on the clinic and the complete medical picture. A young donor with lower AMH may still have good egg quality, but she may produce fewer eggs. If expected egg yield is too low, the clinic may recommend not proceeding with that donor cycle.
4. Do AMH and AFC predict egg quality?
No. AMH and AFC mainly predict ovarian response and expected egg quantity. They do not reliably predict egg quality, embryo quality, pregnancy, or live birth. Egg quality is more strongly related to age.
5. Why are egg donor standards stricter than normal fertility standards?
Because the goal is different. General fertility care asks whether a person may be able to conceive. Egg donor screening asks whether the donor is likely to produce enough mature eggs in one cycle to help intended parents create embryos. That is a higher and more specific standard.
6. Should intended parents request a rematch if AMH or AFC is low?
They should discuss it with the fertility physician and agency. If AMH or AFC is below the clinic’s preferred range, especially in a first-time donor, a rematch may be medically and financially reasonable. The decision should be based on expected egg yield, embryo goals, timeline, and the physician’s recommendation.
7. Can birth control affect AMH or AFC?
Yes, hormonal contraception may lower ovarian reserve markers in some patients. In certain cases, AMH or AFC may improve after stopping hormonal contraception, especially when AFC is low. A fertility physician can decide whether repeat testing is appropriate.
8. Is a first-time donor riskier than an experienced donor?
A first-time donor is not necessarily risky, but there is more uncertainty. Her AMH and AFC can help predict response, but actual egg yield and embryo development are unknown until the cycle is completed. An experienced donor may provide more predictability because prior retrieval results are available.
Sources
- American Society for Reproductive Medicine. Guidance Regarding Gamete and Embryo Donation, 2024.
- American Society for Reproductive Medicine. Testing and Interpreting Measures of Ovarian Reserve: A Committee Opinion, 2020.
- American Society for Reproductive Medicine. The Use of Hormonal Contraceptives in Fertility Treatments: A Committee Opinion, 2024.
- Melo MA, Garrido N, Alvarez C, et al. Antral follicle count can be used in the prediction of ovarian response but cannot predict oocyte/embryo quality or IVF outcome in an egg donation program. Fertility and Sterility, 2009.



