Key Takeaways
- Within BMI 30–32, success rates for embryo transfer remain almost identical to those in normal BMI ranges.
- The largest U.S. study of 56,564 frozen embryo transfers found only small, non-significant differences in clinical pregnancy and live birth rates below BMI 30.
- For gestational carriers, overall health, uterine condition, and pregnancy history matter more than a few BMI points.
- If your IVF doctor’s clinic allows BMI ≤32, a carrier with BMI 31–32 is still a strong and safe candidate.
- Clinics set BMI limits mainly to reduce risks such as gestational diabetes and preeclampsia — not because success rates drop dramatically.
When prospective parents begin their surrogacy journey, one of the first questions they often ask is: “What BMI should a gestational carrier have?” Many fertility clinics in the U.S. recommend a BMI below 30 and sometimes accept up to 32. But does a few points above 30 truly make a difference? Recent evidence from more than 56,000 frozen embryo transfers (FETs) in U.S. clinics suggests that within this range, success rates are nearly identical.
What the Largest U.S. Study Shows
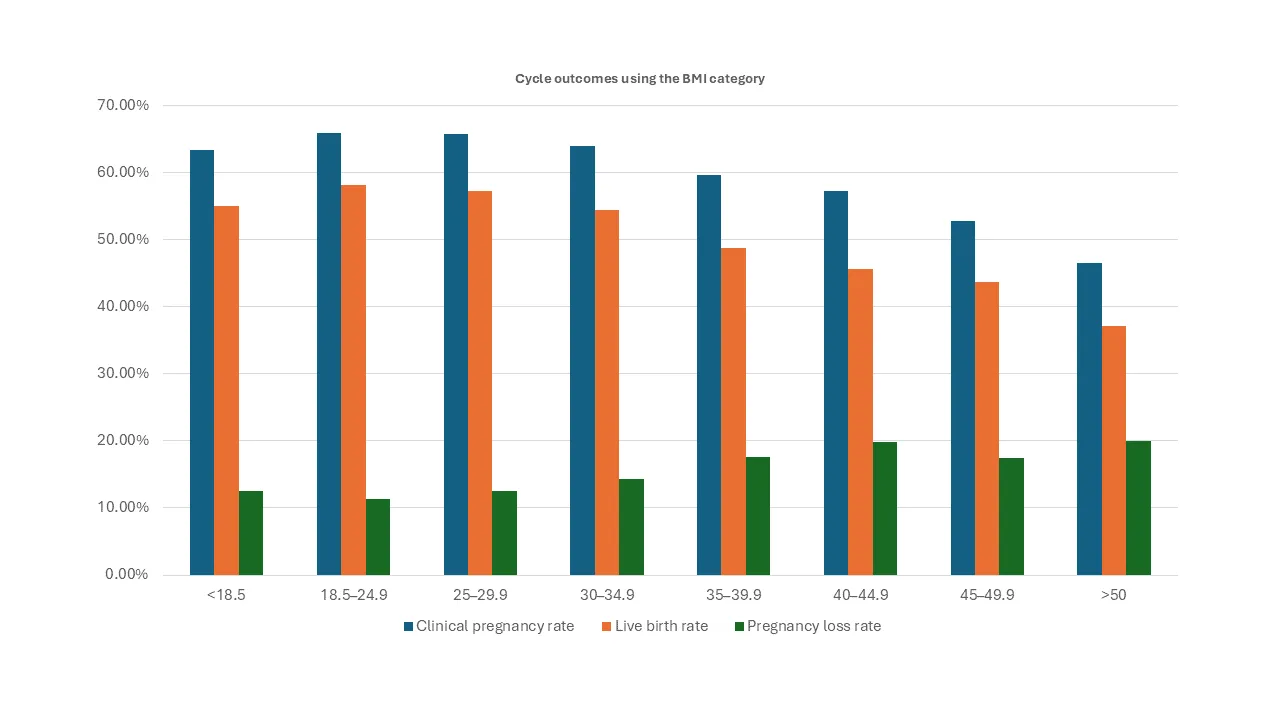
In 2024, Bakkensen et al. published “Frozen embryo transfer outcomes decline with increasing female BMI: Analysis of 56,564 euploid blastocyst transfers” in Fertility and Sterility. This large-scale study examined outcomes of chromosomally normal (euploid) embryos, which removes embryo quality as a variable and focuses instead on the uterine environment and overall maternal health.
The researchers compared outcomes across eight BMI groups:
BMI (kg/m²) | Clinical Pregnancy Rate | Live Birth Rate | Pregnancy Loss Rate |
|---|---|---|---|
< 18.5 (Underweight) | 63.3% | 55.0% | 12.5% |
18.5 – 24.9 (Normal) | 65.9% | 58.2% | 11.4% |
25 – 29.9 (Overweight) | 65.8% | 57.2% | 12.5% |
30 – 34.9 (Class I Obesity) | 63.9% | 54.4% | 14.3% |
35 – 39.9 (Class II Obesity) | 59.7% | 48.8% | 17.6% |
40 – 44.9 (Class III Obesity) | 57.2% | 45.6% | 19.8% |
45 – 49.9 | 52.8% | 43.7% | 17.4% |
≥ 50 | 46.5% | 37.2% | 20.0% |
(Source: Fertility & Sterility 2024; Table 2)
Understanding the Numbers
If we focus on the groups most relevant for gestational carriers—BMI below 30, or even up to 32–34—the differences are minimal:
- Between normal BMI (18.5–24.9) and overweight (25–29.9), clinical pregnancy rates are 65.9% vs 65.8%, virtually identical.
- Live birth rates are 58.2% vs 57.2%, differing by just 1%.
- Pregnancy loss rates differ by only 1 percentage point (11.4% vs 12.5%).
- Even for BMI 30–34.9, clinical pregnancy (63.9%) and live birth (54.4%) remain strong—only slightly lower.
In other words, a healthy gestational carrier with BMI 31 or 32 has nearly the same probability of success as one with BMI 25. Only when BMI exceeds 35 does the risk begin to rise more noticeably.
BMI Matters Less When the Uterus Is Healthy
The same study found that when infertility was due solely to male factors, BMI had little to no effect on outcomes. This means BMI itself isn’t necessarily harmful—what truly matters is the carrier’s overall reproductive and metabolic health.
Because gestational carriers undergo thorough medical screening, they already represent a population with excellent health and low-risk profiles. Mild differences in BMI are unlikely to make a clinical difference.
What This Means for Choosing a Gestational Carrier
At Ivy Surrogacy, we encourage prospective parents to balance caution with perspective. Here’s how the evidence translates into practical, reassuring guidance:
- BMI ≤ 30 is a strong benchmark—but not a rigid rule. A carrier in the 25–30 range has virtually the same chance of success as one with BMI 23 or 24.
- BMI ≤ 32 is still acceptable in many clinics. If your IVF doctor allows up to 32, and your carrier’s BMI is 31 or 32, there’s no need to worry. Just follow your doctor’s recommendation with confidence.
- Beyond 35, proceed with care. Above BMI 35, success rates and pregnancy complications start to diverge more clearly. Most clinics and agencies prefer carriers below this threshold.
- Focus on whole-person health. Factors like blood pressure, glucose level, uterine condition, and previous pregnancies often matter more than BMI alone.
Putting It in Perspective
It’s natural for intended parents to want the best possible carrier—but perfection on paper doesn’t always mean higher success rates. A difference of three or four BMI points rarely determines the outcome of an embryo transfer. What truly counts is a healthy uterine environment, a good medical history, and a trustworthy partnership between intended parents, surrogate, and clinic.
Sometimes, a slightly higher BMI surrogate who has had smooth, uncomplicated pregnancies may actually be the most dependable option.
Frequently Asked Questions
1. What is the ideal BMI for a gestational carrier?
Most fertility clinics prefer BMI under 30, though many accept up to 32. Within this range, studies show nearly identical success rates.
2. Does BMI 29 vs BMI 23 really make a difference?
Not in any meaningful way. In a study of 56,000 transfers, clinical pregnancy rates were 65.9% vs 65.8%. That’s essentially the same outcome.
3. What if my IVF doctor allows BMI up to 32, and my carrier’s BMI is 31 or 32?
You don’t need to worry. If your clinic’s limit is ≤32 and your carrier meets that, you’re still well within the safe and effective range. Follow your doctor’s advice—they know what’s best for both success and safety.
4. What if my doctor requires BMI ≤30, but a potential surrogate has BMI 31 or 32?
Follow your doctor’s guidance. You can either wait for the surrogate to lose a small amount of weight to meet the clinic’s requirement, or choose another candidate who already qualifies. Clinics set these thresholds based on medical safety standards and their own experience with patient outcomes.
5. Is BMI the only factor that matters?
Not at all. A carrier’s prior pregnancy history, uterine health, metabolic screening, and emotional readiness are equally—if not more—important than BMI.
6. Why do clinics have strict BMI limits if success rates are nearly the same?
IVF clinics have two main goals: a successful pregnancy for you, and a safe pregnancy for your surrogate. While the data show the first goal is very achievable even with a slightly higher BMI, stricter BMI limits are designed to protect the second goal—by reducing the risk of complications such as gestational diabetes, preeclampsia, and C-section delivery. These policies are about keeping both the carrier and baby safe and healthy.
Ready to Begin Your Journey
If you’re a healthy woman considering becoming a gestational carrier, we welcome you to apply — even if your BMI is in the low 30s. Your dedication, compassion, and history of healthy pregnancies matter most.
If you’re an intended parent, let our experienced team guide you through the process of evaluating gestational carriers holistically. At Ivy Surrogacy, we collaborate with top fertility specialists nationwide to ensure every match is medically sound, emotionally supportive, and tailored for success.
Reach out today to learn how we can help you move forward — with confidence and peace of mind.
Reference
Bakkensen JB et al. (2024). Frozen embryo transfer outcomes decline with increasing female body mass index in female but not male factor infertility: Analysis of 56,564 euploid blastocyst transfers. Fertility and Sterility, Volume 121, Issue 2, 271 – 280



