Most intended parents tell us their infectious-disease results are "all negative." Most of them are right. But "I think we're fine" and "here is the actual lab report" are not the same thing — and in surrogacy, the gap between the two can cost you a matched surrogate, a signed contract, and tens of thousands of dollars.
This is a plain-English guide to one of the most avoidable — and most expensive — surprises in the surrogacy process: discovering, late in the journey, that an intended parent is hepatitis B positive when everyone believed otherwise. We'll explain what an FDA "ineligible" result really means (it is not a disqualification), why this matters in a special way for intended parents from China, and the one simple step that prevents the whole problem.
Key Takeaways
- A hepatitis B-positive (or other infectious-disease-positive) result does not disqualify you from surrogacy. There is an established FDA pathway for it.
- The danger is not the diagnosis — it's discovering it late, after matching, contracts, and money are already committed.
- Your surrogate is the FDA recipient, and she must consent if a donor is "ineligible." Many surrogates state upfront whether they'll carry for HBV-positive parents.
- Never report your infectious-disease status from memory. Get the actual FDA test report from your clinic and share it with your agency before matching.
- This matters in a special way for intended parents from China, where chronic hepatitis B is common and the FDA framework is usually being encountered for the first time.
A Real Story: "We're All Negative" — Until the Form Said Otherwise
A Chinese couple came to us ready to begin. As we always do — and especially because we work with so many families from China, where chronic hepatitis B is common — we asked directly about their FDA infectious-disease results, hepatitis B in particular. Their answer was firm and confident: no problems, everything negative. When they completed their profile on our platform, every infectious-disease field was marked negative.
Based on that information, we matched them with a wonderful surrogate. Her matching preferences were clear and specific: she was not willing to carry for intended parents with a history of hepatitis B.
Things moved forward, and she passed her medical screening. Then the IVF clinic asked her to sign an informed-consent form. That form was an FDA "ineligible" determination, and it stated that the intended father had tested positive for hepatitis B surface antigen and hepatitis B core antibody.
She had not signed up for this. After a careful phone call with the clinic explaining the actual (low) risk and her options, she decided to go ahead and sign, and the journey continued.
But pause on how close this came to collapse. If she had said no — entirely her right — the intended parents would have lost this match and the time and money already invested in screening her, and would have had to start the matching process over from the beginning. All because a single set of lab results was reported from memory instead of from the actual report.
What an FDA "Ineligible" Result Actually Means (and What It Doesn't)
Here is the part that surprises almost everyone, and the part we most want you to understand:
"Ineligible" is a regulatory label, not a verdict on whether you can have a child through surrogacy.
As we explained in our companion guide, FDA Donor Eligibility Testing for Surrogacy, the gamete providers — the intended father providing sperm, and the intended mother or donor providing eggs — are treated as donors under the FDA's rules (21 CFR Part 1271). The surrogate is the recipient.
Under those rules, a donor whose blood tests reactive for a relevant communicable disease — including a positive hepatitis B surface antigen (HBsAg) — must be classified as "ineligible." The clinic has no discretion to call it anything else; this is a strict requirement, and clinics have been cited by the FDA for getting it wrong.¹
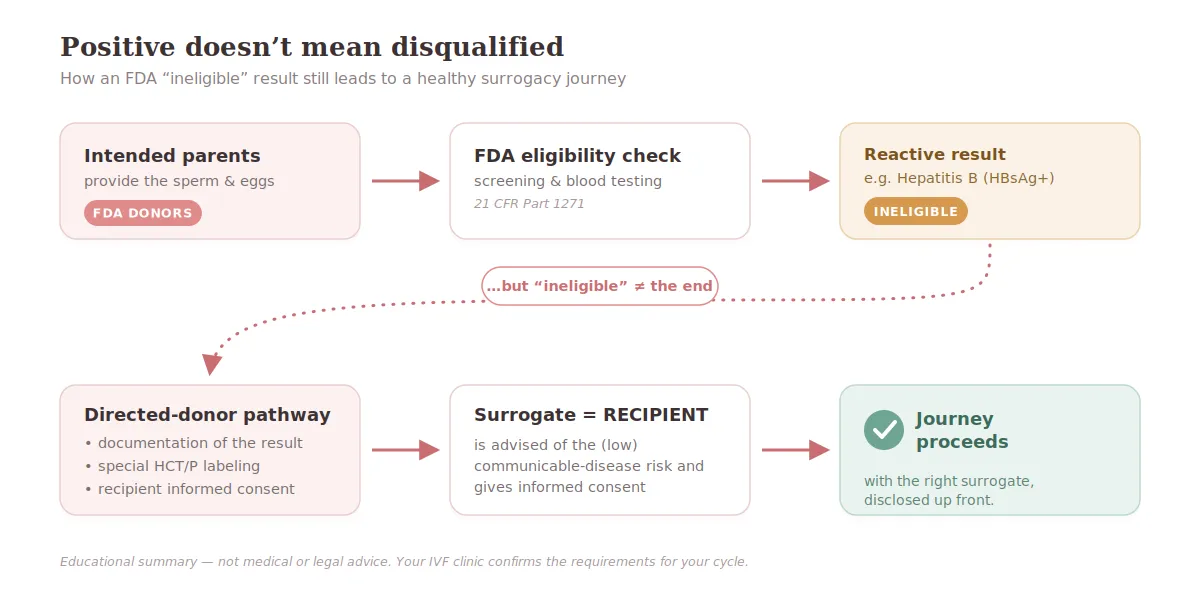
But "ineligible" does not mean your embryos cannot be used. The regulations contain a specific, deliberate exception for directed reproductive donors — which is exactly what an intended father is when his sperm is used to create embryos for a gestational carrier. The FDA built this exception precisely to respect couples who knowingly make a joint decision to have a child.² ³
When this exception is used, three things happen:
- The clinic documents the reason for ineligibility (e.g., reactive hepatitis B test).
- The specimens and embryos receive special labeling noting the ineligible status and the communicable-disease risk.
- The **recipient — your surrogate — is formally advised of the risk and asked to give informed consent.**³
That third step is the form our intended parents' surrogate received. People sometimes call it a "waiver." It is really a consent and acknowledgment that the surrogate is being asked to carry an embryo from a donor who tested positive. This pathway is well established and used routinely. With proper labeling, counseling, and consent, the medical risk to the surrogate is generally considered low — but it's the clinic, not the agency, that should explain the specific risk to her.
The takeaway: a hepatitis B-positive result is not the end of your journey. It is a known situation with a known, manageable process. The danger is never the diagnosis. The danger is the surprise.
Why This Hits Intended Parents From China Differently
We say this with respect and from long experience, not as criticism: among our Chinese intended parents, two things often combine to create exactly this kind of surprise.
First, chronic hepatitis B is genuinely common. China has historically had a high prevalence of chronic HBV. Many people are lifelong carriers who feel completely healthy, whose liver function is normal, and who reasonably think of themselves as "fine." Feeling fine is not the same as testing negative.
Second, most intended parents have never seen the rules before — because they never needed to. If you did IVF for yourselves back home, you and your partner were "sexually intimate partners" in the eyes of these regulations, and partner-to-partner use is exempt from donor-eligibility rules altogether. So the question of "eligible vs. ineligible" never came up. The moment a surrogate enters the picture, she becomes the recipient — someone who is not your partner — and the directed-donor rules apply for the first time. Nothing about your health changed. The legal framework around it did.
Add a third, very human factor: medical terminology is confusing in any language, and even more so across two. Many people don't realize that:
- "I had hepatitis B treated" or "my doctor said it's controlled" is not the same as "negative."
- HBsAg positive (surface antigen) generally indicates a current hepatitis B infection, which may be acute or chronic. On its own it doesn't tell you how active the virus is, or whether your liver function is affected.
- Anti-HBc positive (core antibody) signals that your body has encountered the virus.
- A positive vaccine antibody (anti-HBs) is a good result and means something entirely different.
We'll publish a separate, deeper guide on what each of these hepatitis B markers actually means. For now, the only thing you need to hold onto is this: do not interpret your own results from memory. Get the report.
The Hidden Risk: Your Result Meets Your Surrogate's Wishes
Why does an honest, upfront result matter so much? Because of when the truth otherwise surfaces.
Surrogates are real people with real preferences, and many state clearly — as ours did — whether they are willing to carry for intended parents with an infectious-disease history. We honor those preferences when we match. That is part of protecting both sides.
If your true status is on the table before matching, we simply match you with a surrogate who is comfortable with it. There are many. The journey proceeds smoothly, and the FDA consent form at the end is a formality everyone expected.
If your true status only appears at the clinic's final form — after screening, after the legal contract, after the transfer is scheduled — it can collide head-on with a surrogate who never agreed to it. At that point she has every right to decline. And if she does, you don't just lose time. Depending on your agency's fee structure, you may lose money that is already committed and non-refundable. (This is one more reason to understand how and when agency fees are charged before you sign.)
The diagnosis was never the problem. The mismatch — created by an inaccurate profile — was.
The One Step That Prevents All of This
You don't need a medical degree. You need a document.
✅ Ask your IVF clinic for your actual FDA infectious-disease test report — the one with the test names, collection dates, and results for HBsAg, anti-HBc, HIV, HCV, syphilis, and the rest of the panel.
✅ Send it to your agency before matching, not after — they're the ones matching you, and they can't match around a risk they don't know about.
✅ Don't translate, summarize, or interpret it yourself. Send the report as-is and let your clinic read it.
✅ If you've ever been told you carry hepatitis B, or you're simply not sure, say so early. It changes nothing about your eligibility for surrogacy. It only changes which surrogate is the right match for you — and that's a problem best solved on day one, not on transfer day.
That's it. One report, shared early, removes the single most expensive surprise in this entire process.
Frequently Asked Questions (FAQs)
1) If I'm hepatitis B positive, can I still have a baby through surrogacy in the U.S.?
In nearly all cases, yes. A positive result makes you "ineligible" as a donor under FDA rules, but the directed-reproductive-donor exception allows your embryos to be used with proper documentation, labeling, and your surrogate's informed consent.² ³ The key is matching you with a surrogate who is comfortable with it from the start.
2) Does "ineligible" mean something is wrong with my embryos?
No. It is a regulatory status tied to your test results, not a judgment on embryo quality. This is a recognized situation in fertility practice, and clinics have established procedures for handling it.
3) Why did no one flag this when we did IVF back home as a couple?
Because partner-to-partner reproduction is exempt from these donor-eligibility rules. They apply once a surrogate — who is not your partner — becomes the recipient. It's new to you because the situation is new, not because you did anything wrong.
4) What exactly is the form my surrogate has to sign?
It's an informed-consent and acknowledgment document confirming she understands she is carrying an embryo from a donor who tested positive for a communicable disease, and that she agrees to proceed.³ Clinics typically walk her through the actual (low) risk before she signs.
5) What if I genuinely don't know my status?
Get your FDA test report from your clinic, or ask to be tested. Don't guess, and don't fill in "negative" because you feel healthy. Tell your agency you're confirming — that single sentence protects your entire journey.
6) Will being upfront make agencies or surrogates reject me?
No. It does the opposite — it lets us find the right surrogate for you efficiently and removes the risk of a late-stage collapse. Honesty early is what protects your match.
7) What if only the intended father is hepatitis B positive?
That's one of the most common situations we see. Because the intended father provides the sperm, his result is what drives the FDA "ineligible" determination and the directed-donor consent process — even if the intended mother (or egg donor) is fully negative. The pathway is the same either way: it's manageable, as long as it's known before matching.
8) Does hepatitis B affect embryo quality or the genetic health of the baby?
These are separate issues. Hepatitis B status is an infectious-disease and regulatory matter — it is not a genetic diagnosis, and it is not, in itself, a statement about embryo quality. Questions about embryo quality, grading, or genetic testing belong with your IVF physician and embryology lab.
9) Should I tell the agency before I even have a surrogate match?
Yes — that's exactly the point. The most useful time to share your status is before we start showing you surrogate profiles, because it determines which surrogates are the right fit for you. Disclosing early costs you nothing; it's what keeps your match from falling apart later.
Before You Match: Request a Confidential FDA Lab-Report Review
You don't have to decode your results alone. If you've ever been told you carry hepatitis B — or you simply aren't sure what your test report says — the smartest move is to have it reviewed before matching, not after.

Send us the infectious-disease report from your IVF clinic, and we'll help you understand:
- what your clinic is likely to flag,
- whether any result could affect your surrogate match, and
- what to clarify before contracts or transfer planning begin.
It's confidential, it's early, and it's the single best way to protect both your match and your timeline.
Next step: Request your confidential lab-report review — send us your FDA test report, or let us help you get it from your clinic. We'll make sure your journey starts on solid ground.
Regulatory References
¹ U.S. Food and Drug Administration. Warning Letter — Washington Fertility Center (04/30/2024). Confirms that under 21 CFR 1271.80(d)(1), a donor whose specimen tests reactive (including HBsAg) must be determined ineligible, for both anonymous and directed donors. FDA.gov
² U.S. Food and Drug Administration. Title 21, Code of Federal Regulations, Part 1271, Subpart C — Donor Eligibility (§ 1271.65). Use of an HCT/P from an ineligible directed reproductive donor is not prohibited, subject to labeling and consent requirements. eCFR Link
³ U.S. Food and Drug Administration. Guidance for Industry: Eligibility Determination for Donors of Human Cells, Tissues, and Cellular and Tissue-Based Products (HCT/Ps) (May 2, 2024). FDA.gov
This article is for general educational purposes and is not medical or legal advice. FDA procedures and clinic policies can vary by clinic, by state, and by the specifics of your case. Always confirm the requirements for your cycle with your IVF physician and your reproductive attorney.



